 Welcome
Welcome
“May all be happy, may all be healed, may all be at peace and may no one ever suffer."
Ductal carcinoma in situ (DCIS)
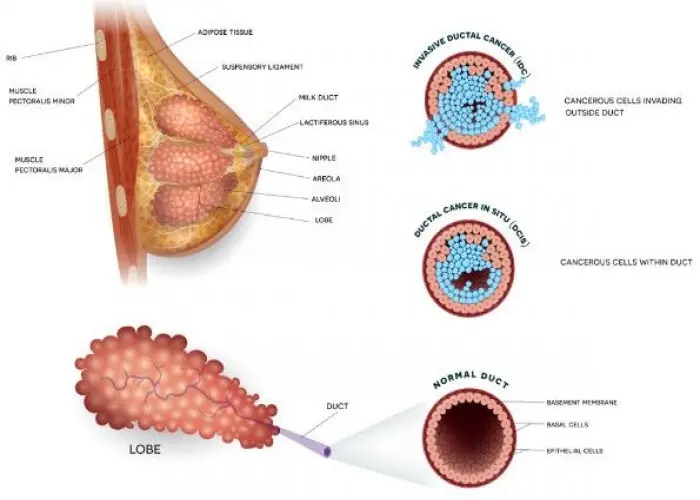
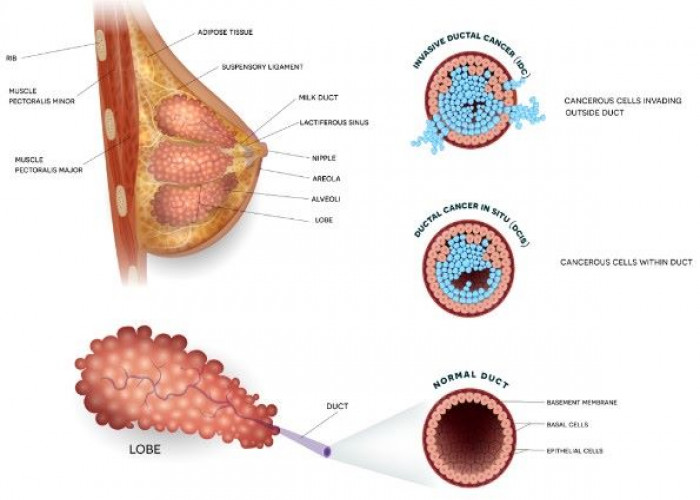
Ductal carcinoma in situ (DCIS) is a non-invasive form of breast cancer in which abnormal cells are found in the lining of the breast ducts but have not spread beyond the ducts into surrounding breast tissue. The word "carcinoma" refers to a cancerous tumor, while "in situ" means that the abnormal cells are contained within the ducts and have not invaded surrounding tissue.
DCIS is typically diagnosed through a mammogram, which may show calcium deposits or a small cluster of abnormal cells in the breast ducts. A breast biopsy may be needed to confirm the diagnosis and determine the stage and grade of cancer.
DCIS is considered to be a pre-cancerous condition, as it has the potential to develop into invasive breast cancer if left untreated. However, many cases of DCIS do not progress to invasive cancer and may not require treatment beyond regular monitoring with mammograms and physical exams.
Treatment options for DCIS may include lumpectomy (surgical removal of the abnormal cells and a surrounding margin of healthy tissue) or mastectomy (surgical removal of the entire breast). Radiation therapy may also be recommended to reduce the risk of recurrence. In some cases, hormone therapy may be recommended to reduce the risk of new or recurrent DCIS.
The prognosis for DCIS is generally excellent, with a high rate of cure and a low risk of recurrence or progression to invasive cancer. However, close monitoring and follow-up with a healthcare professional are essential to ensure that any new or recurrent breast changes are detected and treated promptly.
Research Papers
Disease Signs and Symptoms
- Breast lump
- Nipple discharge
- Bloody nipple discharge
Disease Causes
Ductal carcinoma in situ (DCIS)
It's not clear what causes DCIS. DCIS forms when genetic mutations occur in the DNA of breast duct cells. The genetic mutations cause the cells to appear abnormal, but the cells don't yet have the ability to break out of the breast duct.
Researchers don't know exactly what triggers the abnormal cell growth that leads to DCIS. Factors that may play a part include your lifestyle, your environment and genes passed to you from your parents.
Disease Prevents
Disease Treatments
Treatment of DCIS has a high likelihood of success, in most instances removing the tumor and preventing any recurrence.
In most people, treatment options for DCIS include:
- Breast-conserving surgery (lumpectomy) and radiation therapy
- Breast-removing surgery (mastectomy)
In some cases, treatment options may include:
- Lumpectomy only
- Lumpectomy and hormone therapy
- Participation in a clinical trial comparing close monitoring with surgery
Surgery
If you're diagnosed with DCIS, one of the first decisions you'll have to make is whether to treat the condition with lumpectomy or mastectomy.
- Lumpectomy. Lumpectomy is surgery to remove the area of DCIS and a margin of healthy tissue that surrounds it. This is also known as a surgical biopsy or wide local incision.
- The procedure allows you to keep as much of your breast as possible, and depending on the amount of tissue removed, usually eliminates the need for breast reconstruction.
- Research suggests that women treated with lumpectomy have a slightly higher risk of recurrence than women who undergo mastectomy; however, survival rates between the two groups are very similar.
- If you have other serious health conditions, you might consider other options, such as lumpectomy plus hormone therapy, lumpectomy alone or no treatment.
- Mastectomy. Mastectomy is an operation to remove all of the breast tissue. Breast reconstruction to restore the appearance of you breast can be done at the same time or in a later procedure, if you desire.
Most women with DCIS are candidates for lumpectomy. However, mastectomy may be recommended if:
- You have a large area of DCIS. If the area is large relative to the size of your breast, a lumpectomy may not produce acceptable cosmetic results.
- There's more than one area of DCIS (multifocal or multicentric disease). It's difficult to remove multiple areas of DCIS with a lumpectomy. This is especially true if DCIS is found in different sections — or quadrants — of the breast.
- Tissue samples taken for biopsy show abnormal cells at or near the edge (margin) of the tissue specimen. There may be more DCIS than originally thought, meaning that a lumpectomy might not be adequate to remove all areas of DCIS. Additional tissue may need to be removed, which could require mastectomy to remove all of the breast tissue if the area of DCIS involvement is large relative to the size of the breast.
- You're not a candidate for radiation therapy. Radiation is usually given after a lumpectomy.
- You may not be a candidate if you're diagnosed in the first trimester of pregnancy, you've received prior radiation to your chest or breast, or you have a condition that makes you more sensitive to the side effects of radiation therapy, such as systemic lupus erythematosus.
- You prefer to have a mastectomy rather than a lumpectomy. For instance, you might not want a lumpectomy if you don't want to have radiation therapy.
Because DCIS is noninvasive, surgery typically doesn't involve the removal of lymph nodes from under your arm. The chance of finding cancer in the lymph nodes is extremely small.
If tissue obtained during surgery leads your doctor to think that abnormal cells may have spread outside the breast duct or if you are having a mastectomy, then a sentinel node biopsy or removal of some lymph nodes may be done as part of the surgery.
Radiation therapy
Radiation therapy uses high-energy beams, such as X-rays or protons, to kill abnormal cells. Radiation therapy after lumpectomy reduces the chance that DCIS will come back (recur) or that it will progress to invasive cancer.
Radiation most often comes from a machine that moves around your body, precisely aiming the beams of radiation at points on your body (external beam radiation). Less commonly, radiation comes from a device temporarily placed inside your breast tissue (brachytherapy).
Radiation is typically used after lumpectomy. But it might not be necessary if you have only a small area of DCIS that is considered low grade and was completely removed during surgery.
Hormone therapy
Hormone therapy is a treatment to block hormones from reaching cancer cells and is only effective against cancers that grow in response to hormones (hormone receptor positive breast cancer).
Hormone therapy isn't a treatment for DCIS in and of itself, but it can be considered an additional (adjuvant) therapy given after surgery or radiation in an attempt to decrease your chance of developing a recurrence of DCIS or invasive breast cancer in either breast in the future.
The drug tamoxifen blocks the action of estrogen — a hormone that fuels some breast cancer cells and promotes tumor growth — to reduce your risk of developing invasive breast cancer. It can be used for up to five years both in women who haven't yet undergone menopause (premenopausal) and in those who have (postmenopausal).
Postmenopausal women may also consider hormone therapy with drugs called aromatase inhibitors. These medications, which are taken for up to five years, work by reducing the amount of estrogen produced in your body.
If you choose to have a mastectomy, there's less reason to use hormone therapy.
With a mastectomy, the risk of invasive breast cancer or recurrent DCIS in the small amount of remaining breast tissue is very small. Any potential benefit from hormone therapy would apply only to the opposite breast.
Discuss the pros and cons of hormone therapy with your doctor.
Disease Diagnoses
Disease Allopathic Generics
Disease Ayurvedic Generics
Disease Homeopathic Generics
Disease yoga
Ductal carcinoma in situ (DCIS) and Learn More about Diseases

Male hypogonadism

Gestational diabetes
Familial adenomatous polyposis
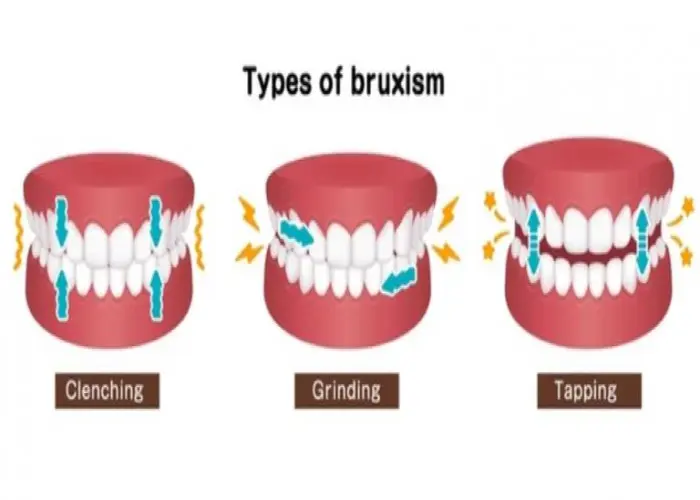
Bruxism (teeth grinding)

Peripheral nerve injuries

Tapeworm infection

Sinus headaches

Vocal cord paralysis
Ductal carcinoma in situ, dcis, ড্যাক্টাল কার্সিনোমা হস সিটু, ডিসিআইএস
To be happy, beautiful, healthy, wealthy, hale and long-lived stay with DM3S.