 Welcome
Welcome
“May all be happy, may all be healed, may all be at peace and may no one ever suffer."
Placenta accreta
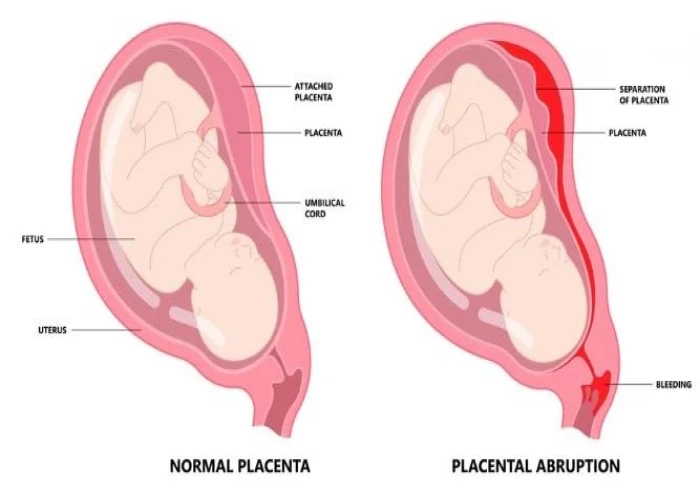

Placenta accrete is a pregnancy complication in which the placenta, the organ that nourishes the fetus during pregnancy, attaches too deeply to the wall of the uterus. This can cause the placenta to remain attached to the uterus after delivery and can lead to severe bleeding and other complications.
The exact cause of placenta accreta is not fully understood, but it is more likely to occur in women who have had a previous C-section, placenta previa, or other uterine surgery, as well as women with certain medical conditions, such as uterine fibroids.
Symptoms of placenta accreta may include abnormal vaginal bleeding during pregnancy, a lack of fetal movement, and an enlarged uterus. Diagnosis of placenta accreta may involve ultrasound imaging and magnetic resonance imaging (MRI) to evaluate the position and attachment of the placenta.
Treatment for placenta accreta may involve the delivery of the baby via cesarean section, followed by removal of the placenta and surgical repair of the uterus if necessary. In some cases, a hysterectomy (removal of the uterus) may be necessary to control bleeding and prevent further complications.
Prevention of placenta accreta involves careful management of high-risk pregnancies, such as those with previous uterine surgeries or medical conditions. Women with a history of placenta accreta should work closely with their healthcare provider to plan for a safe delivery and minimize the risk of complications.
Research Papers
Disease Signs and Symptoms
- Ovaries pain
- Tenderness in the area of your ovaries
- Vaginal pain or burning
- Vaginal bleeding
Disease Causes
Placenta accreta
Placenta accreta is thought to be related to abnormalities in the lining of the uterus, typically due to scarring after a C-section or other uterine surgery. Sometimes, however, placenta accreta occurs without a history of uterine surgery.
Disease Prevents
Disease Treatments
If your health care provider suspects placenta accreta, he or she will work with you to develop a plan to safely deliver your baby.
In the case of extensive placenta accreta, a C-section followed by the surgical removal of the uterus (hysterectomy) might be necessary. This procedure, also called a cesarean hysterectomy, helps prevent the potentially life-threatening blood loss that can occur if there's an attempt to separate the placenta.
If you have vaginal bleeding during the third trimester, your health care provider might recommend pelvic rest or hospitalization.
Before surgery
Your health care team will include your obstetrician and gynecologist, subspecialists in pelvic surgery, an anesthesia team, and a pediatric team.
Your health care provider will discuss the risks and potential complications associated with placenta accreta. He or she might also also discuss the possibility of your:
- Having a blood transfusion during or after delivery
- Needing to be admitted to the intensive care unit after delivery if you have life-threatening bleeding
During surgery
During your C-section, your health care provider will deliver your baby through an initial incision in your abdomen and a second incision in your uterus. After the delivery, a member of your health care team will remove your uterus — with the placenta still attached — to prevent severe bleeding.
After a hysterectomy, you no longer can become pregnant. If you had planned additional pregnancies in the future, discuss possible options with your health care provider.
Rarely, the uterus and placenta might be kept intact, allowing the placenta to dissolve over time. However, this approach can have serious complications, including:
- Severe vaginal bleeding
- Infection
- The need for a hysterectomy at a later date
In addition, limited research suggests that women who are able to avoid hysterectomy after having placenta accreta are at risk of complications, including recurrent placenta accreta, with later pregnancies.
Disease Diagnoses
Disease Allopathic Generics
Disease Ayurvedic Generics
Disease Homeopathic Generics
Disease yoga
Placenta accreta and Learn More about Diseases

Mosquito bites

Heart murmurs
Schizophrenia

Dust mite allergy
Adrenoleukodystrophy

Common warts

Glossitis (Inflammation of tongue)

Jaundice
placenta accreta, প্লাসেন্টা অ্যাক্রেটা
To be happy, beautiful, healthy, wealthy, hale and long-lived stay with DM3S.